There is a discussion to be had about public vaccine policy. The media ought to start having it.
Last week, it was widely reported in the mainstream media that the autopsy of a woman who died of pneumonia earlier this year in the state of Washington found that she had been infected with measles, making this the first confirmed case of measles-related death in the US since 2003. Playing its usual role, the mainstream media is up in arms, blaming the death on parents who choose not to vaccinate their children and telling parents that to not vaccinate is irresponsible. Rather than journalists doing their job by asking hard questions about public policy and seeking out the answers, they choose to act as nothing more than a mouthpiece for government health departments and dutifully tow the official line on vaccine policy.
The woman who died was not among the unvaccinated. On the contrary, she not only had been vaccinated, but reportedly was tested and found to have a protective antibody titer. She nevertheless became infected with measles while seeking medical attention in a clinic. She died from pneumonia, which can be caused by any number of other bacterial or viral infections besides measles, including the common cold and flu. The reason her immune system couldn’t handle the infection was because doctors had her on immunosuppressive drugs. Hence, medical intervention was a contributing factor in her death.
The media, as ever, is pushing the theory of herd immunity to encourage vaccination. Everyone needs to be vaccinated to protect infants and the immunocompromised, we are being told. The argument implies that the individual from whom the deceased caught the measles was unvaccinated, but that is pure speculation; for all we know, the person she contracted the measles virus from had been vaccinated, too.
[pullquote]”It is quite possible for fully vaccinated individuals to get measles.” – Tweet this![/pullquote]
It is quite possible for fully vaccinated individuals to get measles. It is well understood that some people just don’t respond to the vaccine as intended; their immune systems do not produce a great enough amount of antibodies to be considered protective. This is true of about 5 percent of the population, and it’s the reason a second dose, or “booster” shot, is recommended. That second shot is likely unnecessary for most children who did respond to the first, yet it’s given routinely to everyone anyway, even though the purpose is to target the few non-responders. Even after a second dose, however, 3 percent or so of the population still won’t respond.
Moreover, the vaccine-induced immunity, unlike the more robust immunity gained from natural infection, wanes over time. In fact, the CDC considers birth before 1957 to be “evidence of immunity” to measles for the simple reason that pretty much everyone back then was infected with it as a child and gained lifelong immunity as a result.
Also, the measles vaccine is a live-virus vaccine, and individuals can potentially get the disease from the vaccine as well as shed the virus. Vaccine-strain attenuated live viruses can replicate and revert back into virulent form (which is why they don’t vaccinate immunocompromised individuals) or recombine with other viruses to create novel virulent strains. This means that individuals who have received a live-virus vaccine can potentially catch the disease, as well as transmit the virus to others. This is why the live oral poliovirus vaccine was withdrawn from the market in the US, for example; every single domestic case of polio since 1979 was caused by the vaccine.
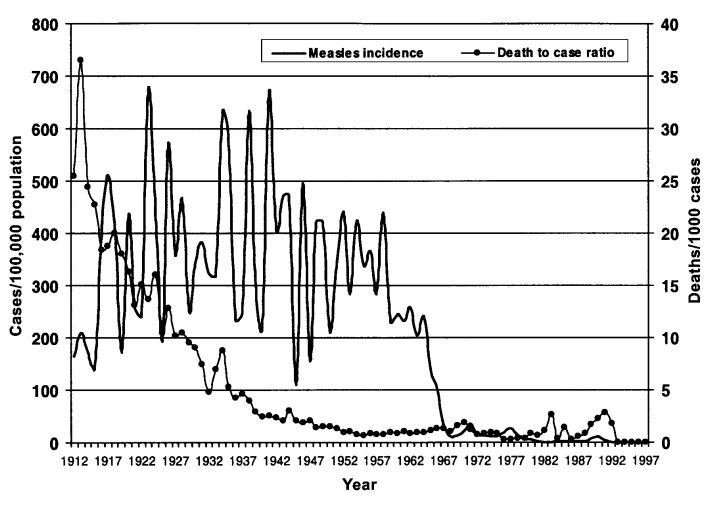
The theory of vaccine-induced herd immunity also overlooks natural herd immunity. Measles is a particularly useful example to illustrate the concept. This is what the measles mortality rate looked like before the introduction of the vaccine:

The vaccine was introduced in 1963, after the latest year shown in the above graph from the US Department of Health. Note that the above graph shows deaths from measles, not incidence of measles, which remained high until the introduction of the vaccine:

In fact, as already noted, it used to be that nearly everyone was exposed to the virus, usually in childhood, and gained lifelong immunity as a result. The virus was still around, but it was becoming less deadly to the US population due to an improving standard of living, better sanitation and hygiene, better nutrition (e.g., vitamin A is important for reducing measles mortality and decreasing morbidity), advances in health care, and so on.
What the declining mortality rate indicates is that the US population was developing natural herd immunity. We were learning to live in symbiosis with the virus, natural exposure to which not only confers permanent immunity to measles itself, but may help prime the immune system of children to protect against other diseases, as well.
But then along came the vaccine and destroyed that natural herd immunity.
While parents today are trained to have a hysterical fear of measles, back in the 1960s, when the vaccine was introduced, it was recognized as a generally mild disease with infrequent complications. In fact, in the era before the vaccine was introduced, it was accepted doctrine that the population would adapt to live in symbiosis with the virus—a respect for the balance of nature that was quickly discarded with the development of the vaccine.
The concept of “herd immunity” today is universally associated with the use of vaccines, but this is an application of the concept in fact borrowed from the observance of natural herd immunity to disease. In the case of measles, researchers in the 1930s—long before the vaccine existed—observed that epidemics in Baltimore occurred in predictable cycles and only when the level of immunity in affected communities was less than 55 percent (far below the 95 percent or so level of vaccination hypothesized to provide herd immunity with vaccination).
Now since nearly everyone is vaccinated at an early age, they don’t become infected with the disease in childhood and hence don’t develop the more robust permanent immunity conferred by natural infection.
[pullquote]”The kind of immunity conferred by vaccines is not the same as that conferred by natural infection.” – Tweet this![/pullquote]
The kind of immunity conferred by vaccines is not the same as that conferred by natural infection. Vaccines favor an antibody response while actually suppressing what is known as cell-mediated immunity. For example, while the flu vaccine offers protection against specific strains of the influenza virus, it works by inducing an antibody response while preventing the cell-mediated immunity that would otherwise offer protection not only against those specific strains of the virus, but other strains as well. Hence, getting an annual flu shot can actually increase the risk of getting the flu. (There are over 200 strains of viruses that cause influenza or flu-like symptoms, the vaccine only targets a handful of them, and public health officials guess each year which ones they think will be in circulation in order to manufacture seasonal vaccines for those specific strains.)
While vaccine theory is premised on the idea of inducing humoral immunity, which involves an antibody response, scientists have learned the production of antibodies is neither always sufficient nor even necessary for the development of immunity.
Since the vaccine-induced immunity from the measles wanes over time, in the event of an outbreak, individuals are at greater risk of developing the disease in their adulthood, when it poses a higher risk of serious complications.
The government and media, of course, blame every outbreak on parents who choose not to vaccinate their children. This was true of the Disney outbreak earlier this year, even though the majority of cases were in adults.
[pullquote]”Measles outbreaks can and do occur in highly vaccinated populations.” – Tweet this![/pullquote]
Measles outbreaks can and do occur in highly vaccinated populations. Even if there was a 100 percent vaccination rate, outbreaks could still occur for the reasons already noted: some individuals do not respond to the vaccine, and the immunity of those who do wanes over time.
Moreover, because of public vaccine policy, mothers today who were never infected during their childhood and hence never developed robust permanent immunity are less able to protect their newborn babies from the disease in the event of an outbreak.
Without the vaccine, women would be infected as children and develop a permanent, robust cell-mediated immunity while continuing to be frequently exposed to the virus, thus also providing a harmless natural boost to their antibody levels. When they become mothers, they would then confer protection to their infants by passing on antibodies through their breastmilk.
But now, since women were vaccinated as children, they likely have a waning antibody titer by the time they start having children. Because the vaccine has quite successfully reduced transmission of the disease, they have not received the beneficial natural boosting of antibodies. Hence, they aren’t able to pass on that antibody protection to their infants.
Public vaccine policy has thus shifted the risk burden away from those in whom the disease is generally well-tolerated and onto those in whom it poses a higher risk of serious complications: adults and the most vulnerable members of society—infants.
Such long-term population-level negative consequences of vaccines simply don’t receive any consideration in the mainstream discussion.
In reports about the measles-related death in Washington, while amplifying public health officials’ recommendation that everyone make sure they and their children have been vaccinated for measles, the media has also failed to even approach the question of the more immediate individual risk associated with the vaccine. When the question of risks does come up, the media tends to treat it as though nonexistent. In the wake of the Disney measles outbreak earlier this year, for instance, the New York Times insisted that there was “no evidence” that vaccines can cause harm and accused anyone who suggests otherwise of being “anti-science”.
This is a puzzling denial, indeed, in light of the fact that, back in the 1980s, the vaccine industry was granted legal immunity by the government because manufacturers were facing so many lawsuits for vaccine injuries that they were going out of business. This in turn threatened public health policy, which prompted the government to step in and bail out the vaccine manufactures by barring consumers from suing them for damages under the National Childhood Vaccine Injury Act of 1986.
Under the law, the National Vaccine Injury Compensation Program was also established to shift the financial burden of compensation for vaccine injuries from Big Pharma to the consumers. The program is funded by a $0.75 tax on every antigen dose of vaccines (so every time an MMR shot is given, being a combination vaccine, $2.25 is taxed for the purpose of contributing to the national vaccine injury fund).
[pullquote]”The Supreme Court has upheld legal immunity for vaccine manufacturers on the grounds that certain adverse reactions are ‘unavoidable’” – Tweet this![/pullquote]
The Supreme Court has upheld legal immunity for vaccine manufacturers on the grounds that certain adverse reactions are “unavoidable” and “design defects” are “not a basis for liability.” Justice Antonin Scalia described this special accommodation for Big Pharma as a “societal bargain”.
The line from the New York Times and other mainstream media that vaccines are harmless is hard to reconcile with the fact that corporations like Merck have been granted legal immunity by the government on the grounds that vaccines are unavoidably unsafe.
As a further illustration of how utterly ignorant and irresponsible such dismissals of the risks associated with vaccines are, one need look no further than the vaccine manufacturers’ product inserts. Merck’s product insert for its measles, mumps, and rubella (MMR) vaccine states that “Unnecessary doses of a vaccine are best avoided….” Surely, there must be a reason? It happens there are many.
For mothers, contraindications to vaccination include pregnancy, as “the possible effects of the vaccine on fetal development are unknown” since there are “no adequate studies” into that question. “However,” Merck appropriately adds, “it would be prudent to assume that the vaccine strain of virus is also capable of inducing adverse fetal effects.” The vaccine-strain mumps virus “has been shown to infect the placenta and fetus”. Studies have shown that the vaccine-strain of rubella virus can be transmitted to infants through the breast milk. Whether this is also true of the measles and mumps viruses “is not known”. Merck advises that “pregnancy should be avoided for 3 months following vaccination” and that “Caution should be exercised when M-M-R II is administered to a nursing woman.” The vaccine also “has not been evaluated for carcinogenic or mutagenic potential, or potential to impair fertility.” Among those who should not receive it are children who are hypersensitive to any of the vaccine’s components, including gelatin and eggs, the latter because the live viruses are propagated in chick embryo cell cultures. The rubella portion of the vaccine is propagated in “human diploid lung fibroblasts”; specifically, WI-38 (ATCC® CCL-75TM), which contaminates the vaccine with human DNA from an aborted female fetus. (This has raised some concern over “ethical problems” at the Vatican; specifically about “cooperation in evil” and the “unjust” practice of forcing parents “to act against their conscience”.) Another ingredient is “fetal bovine serum”. Another is “recombinant human albumin”; specifically, Recombumin® Prime, a product of Novozyems Biopharma US Inc. This is a genetically engineered protein (“recombinant” means it was made by dicing and splicing genetic material). The product was developed because of concerns that using the blood protein albumin from humans or cattle carries the risk of blood-borne contaminants like mycoplasma, prions, or viruses. (This has happened. In March 2010, the rotavirus vaccine Rotarix, manufactured by GlaxoSmithKline, was found to have been contaminated with a pig virus after it was administered to a million children.) Possible adverse reactions to the vaccine include:
- Fever
- Snycope (fainting)
- Headache
- Dizziness
- Vasculitis (a condition in which the immune system mistakenly attacks the blood vessels, causing inflammation that can lead to serious problems, including aneurysms)
- Pancreatitis (inflammation of the pancreas that occurs when the digestive enzymes it produces begin digesting the pancreas itself)
- Diarrhea
- Vomiting
- Parotitis (inflammation of the parotid glands)
- Nausea
- Diabetes mellitus (diabetes)
- Thrombocytopenia (a disorder in which there is an abnormally low amount of platelets, which help blood to clot)
- Anaphylaxis (a life-threatening allergic reaction that can cause cardiac and respiratory arrest)
- Arthritis (joint inflammation)
- Arthralgia (joint pain)
- Myalgia (muscle pain)
- Encephalitis (inflammation of the brain, which can cause permanent brain damage or death)
- Guillain-Barré syndrome (an autoimmune disorder in which the immune system attacks the peripheral nervous system, which can result in paralysis or death)
- Febrile seizures (convulsions brought on by fever)
- Afebrile seizures (convulsions without fever, which may indicate epilepsy)
- Pneumonia
- Measles-like rash
- Death
It is perhaps not too surprising that many of these adverse reactions are the same as the symptoms or complications of wild-type measles itself, including: fever; headache; diarrhea; vomiting; encephalitis; seizures; pneumonia; rash; and, of course, death.
Of course, Merck and public health officials maintain that serious adverse events are rare, less than the risk of developing the same complications from the disease. But, then, the recent case in Washington is the first confirmed case of measles-related death since 2003, while there have been 65 deaths since 2003 reported to the nation Vaccine Adverse Event Reporting System (VAERS) following vaccination with MMR.
Furthermore, the possible adverse reactions listed in the product insert are just a list of known reactions from short-term studies—(and the vaccine manufacturers conduct their own studies to get FDA licensure)—and postmarketing surveillance. The long-term effects of vaccination and its interference in the natural development of an individual’s immune system haven’t been well studied, such as whether vaccination has contributed to the alarming increases in asthma, allergies, and autoimmune diseases.
The continued use of mercury as a preservative in flu vaccines and the use of aluminum as an adjuvant in numerous other childhood vaccines are particularly worrisome practices. Both are known neurotoxins that can pass the placental and blood-brain barriers.
There has never been a double-blind, placebo-controlled study of long-term health outcomes between vaccinated and unvaccinated individuals. As much as the media likes to say that science has shown that there is no risk of developing autism from vaccines, there has never been a study comparing autism rates of individuals who’ve received the CDC’s recommended schedule and unvaccinated individuals.
[pullquote]”Public policy treats vaccination as a one-size-fits-all solution—thus playing Russian roulette with our children.” – Tweet this![/pullquote]
Moreover, it is known that vaccinations can modify gene expression, and certain individuals may be genetically predisposed to having adverse reactions or long-term negative health consequence of being vaccinated; yet public policy treats vaccination as a one-size-fits-all solution—thus playing Russian roulette with our children.
This is all just scratching the surface. The point is that the media treat the subject of vaccines as though there wasn’t even a discussion to be had—just fall in line and get your damn shots! This is dishonest and anti-intellectual. The popular accusation that anyone who questions public vaccine policy is “anti-science” is a particularly hypocritical creed reflective of the intellectual dishonesty and sheer laziness of mainstream journalists who bow to the altar of the state religion and preach official dogma rather than doing their jobs.
Notwithstanding the pretense to the contrary from public health officials and the mainstream media, there is a discussion to be had about public vaccine policy. We ought to start having it.
[Corrections: July 9, 2015: As originally published, this article stated, “There has never been a study of long-term health outcomes between vaccinated and unvaccinated individuals.” This is incorrect. There has never been a double-blind, placebo-controlled study of this kind, which is the “gold standard” of epidemiological studies. The text has been revised to clarify. As originally published, the article stated, “mothers today who were never infected during their childhood and hence never developed robust permanent immunity are unable to protect their newborn babies from the disease in the event of an outbreak.” This is incorrect. Women who have been vaccinated, due to waning immunity, are less able to protect their newborns. The text has been revised to clarify. July 28, 2015: As originally published, this article stated, “In March 2010, the rotavirus vaccine Rotarix, manufactured by GlaxoSmithKline, was found to have been contaminated with a pig virus after it was injected into a million children. Rotarix is an orally-administered live virus vaccine. The error has been corrected.]